Plagiocephaly Update
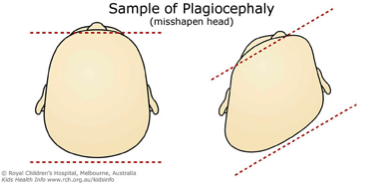
Recent research investigating plagiocephaly (1) has received significant media attention as it found that children treated with helmet therapy did no better than a control group that received education re counter-positioning. However closer inspection of this study indicates a number of flaws which may indeed compromise their results. These flaws included the possibility that the helmets being prescribed were not appropriately fitted, as the study does note that 73% of children experienced issues with the helmet not fitting, and 96% had skin irritation whilst wearing the helmet. This is not the norm for children who receive a helmet in Melbourne.
In contrast Jordan Steinberg and colleagues (2) from the Lurie Childrens Hospital in Chicago followed over 4000 children over a seven year period using a standard treatment algorithm. The children were placed into a conservative group who received education and training regarding positioning and tummy time (RT) +/- biweekly physiotherapy (PT), or a Helmet therapy group, who received a cranial remoulding orthoses (helmet), plus RT +/- PT. Some children in the conservative group who were deemed to not be improving were shifted across to the helmet group.
Complete correction was achieved in 77.1 percent of conservative treatment patients; 15.8 percent required transition to helmet therapy and 7.1 percent ultimately had incomplete correction. Risk factors for failure included poor compliance, advanced age, prolonged torticollis, developmental delay and severity of the head asymmetry at initial examination. Complete correction was achieved in 94.4 percent of patients treated with helmet therapy as first-line therapy and in 96.1 percent of infants who received helmets after failed conservative therapy. Risk factors for helmet failure included poor compliance and advanced age.
At the Victorian Children’s Clinic our Paediatric Physiotherapist Brendan Egan follows a similar treatment programme. Families are educated on the importance of positioning and tummy time, and may also be shown stretches if the child has neck stiffness. Additional developmental sessions may also be required for those children whose development is delayed. We monitor the child until approximately six months of age, when a decision regarding helmet therapy is made. We aim for complete correction using both conservative and orthotic/helmet interventions. For enquiries or to make an appointment please use the contact details above.
References
- Van Wijk, R., van Vlimmeren, L., Groothius-Oudshorn C., Van der Ploeg, C., Ijzerman, M., Boere-Boonekamp, M. (2014) Helmet therapy in infants with positional skull deformation: randomised controlled trial. British Medical Journal, 348:g2741 doi: http://dx.doi.org/10.1136/bmj.g2741
- Steinberg, J., Rawlani, R., Humphries, L., Rawlani, V., Vicari, F. (2015) Effectiveness of Conservative Therapy and Helmet Therapy for Positional Cranial Deformation. Reconstr. Surg. 135: 833-842, doi: 10.1097/PRS.0000000000000955

